

High Rates of Palliative Care Meds in Covid vs non-Covid Patients, Melbourne 2020
High Rates of Palliative Care Meds in Covid vs non-Covid Patients, Melbourne 2020
Sedation for infection control, 'midazolam murders', or something else, like, patient care or disease mitigation?

Many people have expressed concern over the high prescription of palliative care medicine (midazolam) coincident with high numbers of covid deaths. The phrase “midazolam murders” has become a meme.
I write this note to express surprise over the comparatively high use of palliative care medication (un-named) for the symptomatic treatment of covid patients compared with patients with non-covid severe respiratory disease, as detailed in a study, Radcliffe et al, based in Melbourne, Victoria, Australia, in 2020, published in 2022.
In brief, Radcliffe et al was a prospective study that collected data on patients referred by Residential Aged Care Facilities (RACFs) for InReach assistance. I understand that InReach refers to specialist teams treating in the RACF where possible with the dual aims of treating patients in their home environment for patient care reasons, and also for limiting hospital emergency visitations.
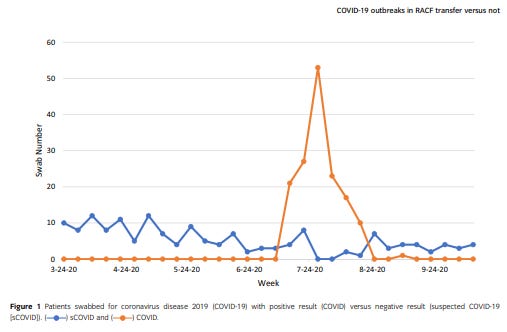
Across the period between 29 March and 13 October 2020 Radcliffe recorded data of patients who tested positive for covid, and patients who had the advisory symptoms of covid (typically respiratory symptoms and fever), but tested negative. While the non-covid patients arrived at a modest level throughout this period, this team were only notified of covid patients through Melbourne’s second covid wave, in winter 2020.
There were 118 non-covid patients, median age 87, of whom 32 died (27%). Post-pub Edit: It is assumed by Radcliffe that the referrer deemed the patients to be sufficiently severe to require InReach services, although their severity scores are comparable to the covid patients.
There were 152 covid patients, median age 88, of whom 35 died (23%). They were of all range of initial severity (from broad testing after first notification), including 12% who remained asymptomatic throughout. Some aged and frail people can clearly be lucky with covid.
Of the non-covid patients, 20 (17%) were referred for “Community palliative care” and 38 (33%) received palliative care medication. ‘Anticipatory’ prescription was provided in respect of 17 (15%).
This InReach team didn’t have full data on all its covid patients - some had already been transferred to other hospitals before they were notified. So the following data on symptomatic management only refers to 137.
Of these 137 covid patients, 27 (20%) were referred for “Community palliative care”, similar to the non-covid patients, but 96 (70%) received palliative care medication, as opposed to 33%. ‘Anticipatory’ prescription was provided in respect of 60 (44%), as opposed to 15%
So, in the non-covid patients, 97% of whom had respiratory symptoms and/or fever serious enough to call for hospital InReach services, 38 received palliative care medication, and 32 died, with 20 referred for palliative care.
In the covid patients with data (of all range of initial severity), 96 received palliative care medication and 35 died, with 27 referred for palliative care.
That’s a huge discrepancy in the use of palliative care medication for symptomatic management of covid patients.
The authors noted the discrepancy, despite similar rates of mortality between their two groups, and seemed to explain it more as a heightened service, rather than an unexpectedly biased management…
A far greater percentage of covid patients ended up with transfer to hospital for patient acuity reasons - 31 of 152 (20%) - as opposed to 5 (4%) for the non-covid patients.
(NB: There were an additional 17 covid patients transferred to hospital for ‘public health’ reasons such as infection control.)
There seemed to be a greater willingness to have non-covid patients die in the RACF (30 out of 32 deaths), compared with the covid patients (16 out of 35 deaths).
Perhaps the palliative care medication in the RACFS was for sedation to assist with infection control?
As someone working through the confounding variables associated with covid death I have to consider to what extent the comparatively high use of midazolam played a role, and also, to what extent it may have helped - I have no expertise on drugs.
The use of palliative care medication wasn’t mentioned in the post-vaccination era Yap et al study, also based in Melbourne, that I’ve referenced in four of my recent substacks.
I have searched within various Australian Guidelines for the care of covid-19 patients, and not found anything specific to this question, yet. If you see something, say something.
The end.
There were more drugs used than midazolam, mind you. But cheers!
I cannot find the conflicts of interest on the Radcliffe study and without those to me it is most likely propaganda. Over 90% of "science" in the medical journals is wrong and cannot be replicated so it is best to wait for confirmation from multiple independent studies before considering anything fact.