


Can a covid vaccine save a life?
Is 15% covid mortality a vaccine win? Pre-thinning the vaccinated cohort to the strongest herd is a strategy, I suppose...

[Best reading: In your browser about half an hour after it arrives in your email box]
*** Please see the “Reprise” substack - more information - here. The authors silently published that 2 Doses did not significantly advantage the frail elderly on Death over their unvaccinated companions.
The Dilemma
I faced a dilemma early in the vaccine rollout… Do I letterbox my town about the high risk of the vaccines, or not? I’ve done this before when the stakes were high on various issues.
The problem was, as risky as the vaccines were, I didn’t have any data on their possible benefits. Could they save someone’s life from covid? I didn’t know.
I knew the Regulators wouldn’t have any data to use apart from that provided from corporations with heinous records of fraud, and there was obviously no publicly available, independent, trustworthy hard data either.
Although there were probably ways I could’ve safely made the communication, I was wary about dissuading someone from a vaccine that could possibly help them. And so I restricted my communications to more official channels, and that cesspit, twitter.
On multiple occasions I made local requests for data, all ignored.
Data slowly arrives, but is inadequate
Some jurisdictions began to publish data, in various forms, but none of it was helpful. Published studies eventually arrived but all had the same fundamental flaws...
One can’t accept the life-saving efficacy claims if the people who died between the vaccines and the first positive covid test weren’t included in the equations. If one has pre-thinned the vaccinated cohort down to the strongest herd it’s hard to subsequently claim the ‘vaccine’ has saved them from covid.
One can’t accept the life-saving efficacy claims if we don’t learn whether the vaccines accelerated transmission/infection in those who were vaccinated.
And, one can’t accept the life-saving efficacy claims without knowing, in respect of the unvaccinated cohort, why the people who were frail enough to die of covid weren’t given the injections.
I’m sure the readers would already have a few ideas about this.
But to the Covid Vaccine Believers, who live in the “vaccines save lives” paradigm... These frail elderly are the people whose lives we valued so much that we denied them visitors and locked ourselves down for months. And now, their lives are suddenly so unimportant that someone forgot to vaccinate them?
The conundrum of unvaccinated elderly
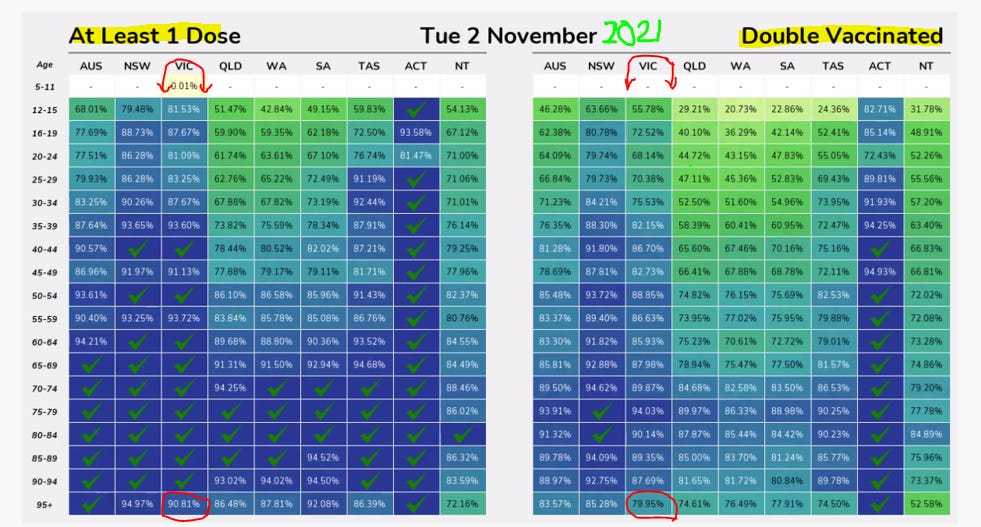
This point is such a conundrum for me, because at the time when vaccines were being mandated in Victoria on any worker outside the home, the vaccination rates of the oldest cohort were actually a lot lower. What’s going on here, Covid Vaccine Believers?
Reasons for not vaccinating a frail elderly person
There are two reasons I can see for not vaccinating a frail elderly person.
The first is that you want them to live, and you are concerned about the vaccine killing them, as reported from Norway before the Australian rollout commenced.
And the second is that, in the absence of flu, covid has assumed the mantle of “the angel of mercy”, and someone in the care plan/medical/power of attorney team has considered that withholding a liquid-gold life-saving vaccine is the merciful thing to do.
When cohorts of the elderly are separated into vaccinated and unvaccinated we thus have a fair idea that the unvaccinated cohort is in a frailer situation than the vaccinated.
There is a third possible reason, being that the vaccinators had not yet arrived at the Retirement Aged Care Facility of the frail elderly person. And a fourth, being that the elderly person has applied their right to medical choice and rejected the vaccines.
But in this study based in my home state by Yap et al, presented below, these third and fourth options seem unlikely

The incentive
I’d generally given up on reading efficacy studies (would a journal even publish a “Nah, the vaccines were useless” study?), but a “lower mortality rate” wasn’t the typical strong language, and “Further research” seemed a little qualifying. I was interested because it was local, and I could relate to it.
Similar to most ‘interesting’ studies, the full text was behind a pay wall, but there was an open-published Editorial that referred to the paper.

In RACFs in Victoria, the covid mortality was not the 0.1% of the Diamond Princess cruisers. A solid 15% mortality in vaccinated covid-positive cases was quite a high death return for vaccine investment.
And then, in my reading, this Editorial statement actually inferred that the vaccines weren’t fit for purpose. In Yap et al’s case the pertinent covid variant was Delta - as closely matched to the genetic injection for the Wuhan variant as researchers were going to get in the Australian rollout.
So I thought that maybe Yap et al would be a full text worth accessing.
The study
The study was a retrospective audit on data from Residential Aged Care Facilities (RAFS) in respect of outbreaks between 9 September and 9 December 2021, in North Melbourne, Victoria. This was when Victorians had utterly tired of lockdowns and Delta was finding its way around. All workers outside the home had been mandated to have their first vaccine by October 16, and their second by early December. Only seriously-vaxed Victorians were allowed in the public space.
And yet there was an unvaccinated cohort of frail elderly in RACFs in Northern Melbourne! Actually, this category was not “unvaccinated” as the Editor said, but rather “Not Fully Vaccinated” - it included 11 people who’d had one vaccine.
(And suddenly there’s a fifth reason that someone might be more at risk from death - weakened by an adverse reaction to a first vaccine.)
Exclusions and Inclusions
Anyway… The study excluded anyone under 65, only included residents with a positive covid test, and the criteria was death from “any cause” within 28 days of the test.
(I thought the “any cause” qualification was strange because anyone who died “with covid”, died “from covid”, in those days. The more I think about that, the weirder “all cause” with a positive covid test gets. Surely they’d know if their resident was given the covid cause of death? Are they qualifying for the higher percentage of people with metastatic cancer in the Not Fully Vaxd group?)
Lives and Deaths
There were 158 people in the Fully Vaccinated cohort (89% Pfizer and 11% Astrazeneca) - 24 sadly died (15%).
There were 33 people in the Not Fully Vaccinated cohort (22 with no vaccines and 11 with one (9-2 Pf-Az)) - 13 sadly died (39%). It seems worse, yes, but read on…
My Purpose
It was clear very early that I wasn’t going to learn how many people died as a consequence of the vaccination process (pre-thinning of the cohort), nor anything about comparative infection rates. As such, questions on vaccine Efficacy against death would be undetermined.
But what I was hunting for was some evidence that the NFV cohort was frailer and more likely to die of covid, exposing the presented Efficacies as being thus biased.
The Clinical Frailty Scale
The researchers collected a great deal of data on many health and morbidity variables. I was surprised to read that the vaxd cohort were older, so this wasn’t going to help my case. According to their statistics most variables were comparable, until I got to the “Clinical Frailty Scale”.
The residents were rated on the CFS at 6, 7 or 8. What do these mean, I wonder? No 9 and 10s? No 1-5s?
The NFV cohort had 10 residents at the highest score of 8 (30%). I thought that if 8 means “bad”, and 13 died in total with 10 at “8” that could explain a lot.
The FV cohort had 29 residents at the highest score of 8 (only 18%), and that was also similar to their death number of 24.
“Typically they could not recover even from a minor illness”
The reference (Rockwood et al) they gave for this Score seemed out of date, but this scale is plastered all over google images.

All of the RACFs residents in this study were very frail, with even the strongest (at 6) maybe needing assistance with bathing and dressing.
But in case you can’t read “8”…
8: LIVING WITH VERY SEVERE FRAILTY: Completely dependent for personal care and approaching end of life. Typically they could not recover even from a minor illness.”
Is Covid a “minor illness”? Anyway, I think we can explain most of the deaths in the Not Fully Vaccinated category, and note a few miracle (or miscategorised) survivors in the Fully Vaccinated category.
A little bit of fudging?
So… Why didn’t this come out in the analysis of the final data? Why wasn’t this clear difference in CFS controlled for?
Well, for some reason, the researchers decided that inclusion in a multivariable analysis required an initial “p value” below 0.20 on the univariable analysis. And, if I’m reading this correctly, the Clinical Frailty Scale was at 0.23, and as such, wasn’t included.
I might write a letter to the researchers on that one, and perhaps the publishers, because I think the CFS was a likely variable of significance in the outcome.
But I think those researchers are inherently good, or at least, have a gnawing conscience, because this popped out in the discussion… I think they know…
“The retrospective nature of the study also means interpretation of records could be subjective amongst investigators (e.g., scoring of CFS).”
I think they also know there is a reason why the unvaccinated weren’t vaccinated…
“Not included in this study were the goals of patient care or advanced care plans, which can significantly influence clinical decisions such as provision of intervention and hospital transfer.”
The End.
I liked your story of the letterboxing. I did that in my community and got death threats while the murderers said that they were the victims and hid from the public.
But the booster uptake tells the story. People are not injecting anymore, and as for those in the vaccine religion, no data will convince, because beliefs are not subject to data.
There's a good reason, within the mainstream medical paradigm, for not vaccinating the very frail elderly: vaccine efficacy depends on having a functional immune system. Plus of course the higher risk, which no health practitioner dares to mention out loud these days. I'm not sure to what extent that was the actual reason for not vaccinating this group - we know now that these decisions are not always made with the patient's benefit in mind. But it's not necessarily sinister.
Of course, that doesn't alter the fact that any study ought to control for this, or at least mention it.
Or that the risks and benefits are inextricably tied together, in determining safety and efficacy as an overall outcome.
And it doesn't alter the fact that they were mindlessly repeating the "safe and effective" mantra before it was possible to know this, and that the precautionary principle - one of the cornerstones of proper medical treatment - would dictate that you would indeed have been justified in letterbox dropping! (Whether it would have been wise is another question - because by that point, most people were so terrified of getting covid and so brainwashed by the "vaccines are going to save us" narrative that they would only have turned on you in fury.)