

Really? All the Deaths were to Covid?
Really? All the Deaths were to Covid?
I didn't expect to be here. I know others have been here before me. But this comes to a completely independent question from a completely independent path of inquiry.

The Path of Wonder
It doesn’t make sense to me…
We know that the older one gets, the more likely one is to die of covid.
Here in Victoria the Chief Health Officer often called the people who died of covid “the very frail” .
And so, I’ve been expecting to find higher rates of covid deaths as the frailty increases.
But studies in Victoria aren’t reporting this. Yap et al found no association between covid death and frailty in their univariate analysis, against Delta in 2021. I was a bit mad at them for not including the variable in multivariable analysis. Relevant substacks here and here.
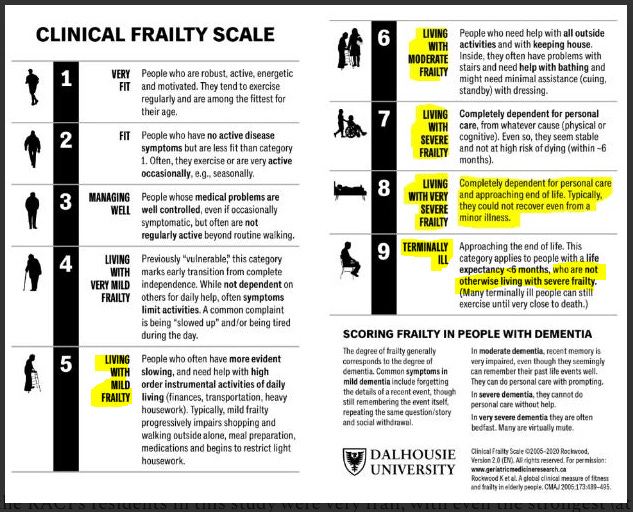
Radcliffe et al used two frailty scales in its analysis - the same “Clinical Frailty Scale” (CFS) that Yap used, and another called FRAIL-NH. They also reported no covid association with Frailty. They almost seemed frustrated or exasperated, saying “We recorded near-universal frailty by CFS, questioning the discriminatory utility of low CFS categories within our population”.
The logical consequence implied that people of all the frailty categories from 5-8 were equally susceptible to Covid deaths. This is despite the fact that Category 8 contains the description “Typically, they could not recover even from a milder illness”. (There’s a category “9” - Terminal - but these are defined as people “not otherwise living with severe frailty”.)
So what did Radcliffe et al associate with Covid death? Only three indicators - Initial Oxygen Saturation, Delirium, and Patient Acuity (ie, the severity of the illness). Almost like saying, if you reacted badly to Covid, you were more likely to die. It’s not a big statement, is it? The logical consequence of that is that death to Covid in the universally frail is chance, only.
In the meantime there was a different blaring signal in the study that I thought I’d write about…
Palliative Care Medication for “Management (symptomatic)”
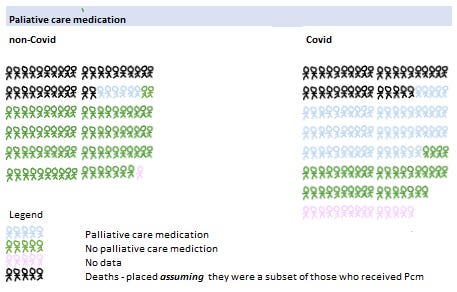
Radcliffe et al compared two groups - a non-Covid group (Covid respiratory and fever symptoms but testing negative), and a Covid group (testing positive). There was a HUGE difference in the percentage of Covid patients who were given palliative care medications, supposedly for symptom management, and yesterday I substacked about it. High Rates of Palliative Care Meds in Covid vs non-Covid Patients, Melbourne 2000. In image form, this is what it looked like:

The probability of that was p = <0.001

Assuming the deaths were a subset of those who received Palliative care medication (I don’t have data on this), the image is as follows:
Explain that.
Frailty was Significant in non-Covid Death
I was reflecting and comparing these two groups. Studies don’t report everything, and without the patient data one can’t do a lot of exploring.
But I suddenly realised that there was enough data to reverse engineer the odds ratios to work out how many people died in each frailty grouping (Radcliffe used <7 and >6) for the Covid and non-Covid groups, coming up with the following:

So, for the Covid patients, the risk of dying for people in the frailest grouping was 27%, and in the less-frailer grouping, 22%, and the OR = 1.3 (0.6 - 3.1) as reported, no significant difference.
But for the non-Covid patients, the risk of people dying in the frailest grouping was 39%, and in the less frail, only 21% with the OR = 2.4 (1.0 - 5.5) , p = 0.04. That was a significant difference.
Frailty made a difference in non-Covid respiratory-type death. And then I set back to wondering why it wasn’t significant in a Covid type of death. And then I wondered if the Palliative care medicine could be over-riding the frailty signals. Radcliffe reported the usage prevalence of Palliative care medication by Covid/non-Covid category, but they did not include it in their analysis. They didn’t control for it.
But everything must logically fit
If the Palliative care medicine (Pcm) was involved in promoting death there would have to be a logical path to Radcliffe’s findings, and there was. It wasn’t hard… Assuming Midazolam was the principal Pcm google search “Midazolam Oxygen Saturation” and discover that O2 suddenly drops with Midazolam. Google search “Midazolam Delirium” and discover that Delirium is one of the side effects.
I think Radcliffe et al need to get their data out again and put Frailty and “Palliative care medicine” along with death and patient acuity into a multivariate analysis for the Covid patients.
If it’s true…
If it’s true that there is an effect between Death (to Wuhan strain covid) and the use of Palliative care medicine (for symptom management) it might be that the Wuhan strain of covid was not nearly as serious as it was made out to be.
In the frailest category the risk of death to Covid was already lower than the risk of death to non-Covid, 27% compared with 39%, (though not significantly). If the Palliative care medicine made it worse than it really is, then, the actual covid risk in that frailest grouping would be even lower than this. But again, small numbers, random variation, not significant.
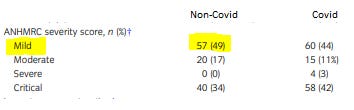
Radcliffe might rebut the idea that Covid was milder than non-Covid, given their statement that they were only notified of patients who were deemed to be “sufficiently severe”.

However this is contradicted by their data on their ANHMRC severity score, with the majority of their patients being in the Mild and Moderate categories, and comparable with Covid.
Rather than try to solve the dilemmas of their findings with logic, as I am limited to, I think they should go back to their data and do some controlled analysis.
The End.
Post publication addition: I don’t have data to preclude the possibility that the palliative care meds were overall helpful, rather than damaging. I’d need data on early Covid with and without palliative care meds, which I don’t have.